English
English Español
Español Français
Français Deutsch
Deutsch Italiano
Italiano Português
Português
Monkeypox has emerged as a Public Health Emergency of International Concern1. From May through July, more than 17,300 confirmed and suspected cases of monkeypox have been identified in all six World Health Organization (WHO) regions. Outbreaks have been identified primarily among men who have sex with men2. As of 11 August, the Centers for Disease Control (CDC) there were 10,768 confirmed cases of monkeypox in the USA3. The WHO is collaborating with health authorities to prevent the further spread of the disease4. They are issuing guidance to help countries with surveillance, laboratory work, clinical care, infection prevention and control. They are also communicating risks to the general public about monkeypox and how to keep safe. They are also working closely with countries in Africa, regional institutions, and technical and financial partners. They aim to improve laboratory diagnosis, disease surveillance, readiness and response actions to prevent further infections4.
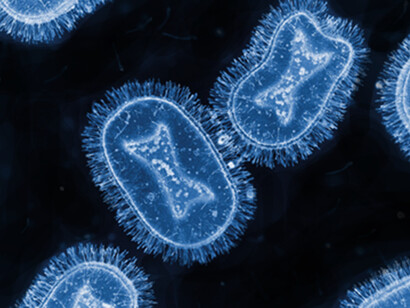
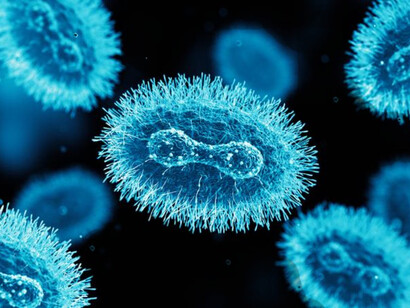
Monkeypox is a rare zoonotic disease, caused by a double-stranded DNA virus belonging to the Orthopoxvirus genus, the Poxviridae family and the Chordopoxvirinae subfamily5. It is closely related to the variola virus, the causative agent of smallpox. Monkeypox was discovered and identified in 1958 in Denmark by the virologist Preben Christian Alexander von Magnus6. He was investigating two outbreaks of diseases in cynomolgus monkeys that resembled smallpox. It is endemic in Africa. No cases outside of the African continent had been reported until 2003, when the importation of infected rodents and exotic animals from Ghana resulted in a cluster of 47 confirmed/probable monkeypox cases in the USA, after the contamination of some pet prairie dogs.
Human monkeypox was not recognized as a distinct infection in humans until 1970 during efforts to eradicate smallpox when the virus was isolated from a patient with suspected smallpox infection in The Democratic Republic of the Congo6. The virus that causes monkeypox can infect many mammalian species. The extent of viral circulation in animal populations and the precise species that may harbor the virus are not known, although several lines of evidence point to rodents as a likely reservoir. Human infections have been linked to contact with animals through household rodent infestations and the hunting or preparation of bush meat from a variety of species. Transmission is thought to occur primarily through saliva and respiratory excretions or contact with exudate or crust material from lesions.
People with monkeypox get a rash that may be located on or near the genitals or anus and could be on other areas like the hands, feet, chest, face, or mouth7. The rash will go through several stages, including scabs, before healing. The rash can initially look like pimples or blisters and may be painful or itchy. Other symptoms of monkeypox can include fever, chills, swollen lymph nodes, exhaustion, muscle aches, backache, headache, and respiratory symptoms (sore throat, nasal congestion, or cough). Patients may experience all or only a few symptoms. Sometimes, people have flu-like symptoms before the rash. Some people get a rash first, followed by other symptoms. Others only experience a rash. Monkeypox symptoms usually start within 3 weeks of exposure to the virus. If someone has flu-like symptoms, they will usually develop a rash 1-4 days later. Monkeypox can be spread from the time symptoms start until the rash has healed, all scabs have fallen off, and a fresh layer of skin has formed. The illness typically lasts 2-4 weeks.
The median age at presentation has increased from 4 (the 1970s) to 21 years (2010–2019)8. There was an overall case fatality rate of 8.7%, with a significant difference between clades (Central African 10.6% and West African 3.6%). Interactions with infected animals or individuals are risky behaviors associated with acquiring monkeypox. There has been an increase in the number of monkeypox cases, especially in the highly endemic DRC. These findings may be related to the cessation of smallpox vaccination, which provided some cross-protection against monkeypox. This caused more transmission between humans.
Even though the mortality of monkeypox is low, it can be excruciating. Some patients compare the pain to glass shards scraping against the skin. Even though the virus is mostly afflicting men who have sex with other men now, that could change if it continues to spread unchecked. Monkeypox mostly spreads through close physical contact, typically skin-to-skin touch. Most infections in the current outbreak have occurred through close contact during sex. Still, the virus can also spread through contaminated surfaces, including clothes and bedding. Brief contact, like a handshake, is usually not enough to spread the virus. Unlike the SARS-CoV-2 virus that causes Covid-19, it does not seem to spread much through the air.
Even though the current outbreak is disproportionately affecting men who have sex with men, monkeypox is no more a “gay disease” than it is an “African disease.” It can affect anyone9.
In a recent study of infections across 16 countries from April – June 2022, the clinical outcomes were reassuring. Most cases were mild and self-limited, and there were no deaths. Although 13% of the people were admitted to a hospital, no serious complications were reported in the majority of those admitted. Common reasons for admission were pain and bacterial superinfections9.
Even though most patients don’t require medication, antivirals such as tecovirimat may be recommended for people who are more likely to get severely ill, like patients with weakened immune systems10.
The CDC recommends vaccinations for people who have been exposed to monkeypox and people who may be more likely to get monkeypox11. People more likely to get monkeypox include:
People who have had contact with someone who has monkeypox People who are aware that one of their sexual partners in the past 2 weeks has been diagnosed with monkeypox People who had multiple sexual partners in the past 2 weeks in an area with known monkeypox People whose job may expose them to orthopoxviruses, such as:
- Laboratory workers who perform testing for orthopoxviruses;
- Laboratory workers who handle cultures or animals with orthopoxviruses;
- Some designated healthcare or public health workers.
The preferred vaccine to protect against monkeypox is jynneos, which is a two-dose vaccine. It takes 14 days after getting the second dose of jynneos for its immune protection to reach its maximum. The acam2000 vaccine may be an alternative to jynneos. acam2000 is a single-dose vaccine, and it takes four weeks after vaccination for its immune protection to reach its maximum. However, it has the potential for more side effects and adverse events than jynneos. It is not recommended for people with severely weakened immune systems and several other conditions.
Acam2000 is administered as a live Vaccinia virus preparation that is inoculated into the skin by pricking the skin surface12. Following a successful inoculation, a lesion will develop at the site of the vaccination. The virus growing at the site of this inoculation lesion can be spread to other parts of the body or even to other people. Individuals who receive vaccination with acam2000 must take precautions to prevent the spread of the vaccine virus and are considered vaccinated within 28 days.
Jynneos is administered as a live virus that is non-replicating. It is administered as two subcutaneous injections four weeks apart. There is no visible lesion and no risk for spread to other parts of the body or other people. People who receive jynneos are not considered vaccinated until two weeks after they receive the second dose of the vaccine.
The U.S. Department of Health and Human Services is increasing the availability of vaccines to over 1.1 million doses13.
Notes
1 Nuzzo, J.B. et al. The WHO declaration of monkeypox as a global public health emergency. JAMA, 27 July, 2022.
2 WHO Multi-country monkeypox outbreak: situation update. June 27, 2022.
3 CDC 2022 U.S. map & case count. 11 Aug., 2022.
4 World Health Organization Monkeypox outbreak 2022.
5 Bragazzi, N.L. et al. Epidemiological trends and clinical features of the ongoing monkeypox epidemic: a preliminary pooled data analysis and literature review. Journal of Medical Virology, 12 June, 2022.
6 McCollum, A.M & Damon, I.K. Human monkeypox. Clinical Infectious Diseases, volume 58, 260-267, 2014.
7 CDC Monkeypox signs and symptoms. 5 Aug., 2022.
8 Bunge, E.M. The changing epidemiology of human monkeypox - a potential threat? A systematic review. PLoS Neglected Tropical Diseases, volume 16, article e0010141, 2022.
9 Thornhill, J.P. et al. Monkeypox virus infections in humans across 16 countries. April – June 2022. New England Journal of Medicine, 1 Aug., 2022.
10 CDC Monkeypox treatment. 10 August, 2022.
11 CDC Monkeypox vaccines. 5 August, 2022.
12 CDC Monkeypox and Smallpox Vaccine Guidance. 2 June, 2022.
13 HHS expands availability of monkeypox vaccine to more than 1.1 million doses. 28 July, 2022.